Medical Authorization Form Medical Consent Authorization
Instructions for completing the authorization for release of health information under the hipaa (oca-960) these instructions will help you to complete the authorization for release of health information under the hipaa (oca-960). it is important authorization for release of health information oca 960 that you read each line of the form carefully and that you make sure you fill in each box correctly. Instructions for completing the authorization for release of health information under the hipaa (oca-960) these instructions will help you to complete the authorization for release of health information under the hipaa (oca-960). it is important that you read each line of the form carefully and that you make sure you fill in each box correctly. Download or email oca 960 & more fillable forms, register and subscribe now!. Oca official form no. : 960 authorization for release of health information pursuant to hipaa [this form has been approved by the new york state department of health] patient name date of birth social security number hamidanmajiamad 9/15/45 patient address 9346 20th street queens village, ny 11428.
Health information management department suny downstate.

Pcr Request Bay Shore Brightwaters Rescue Ambulance
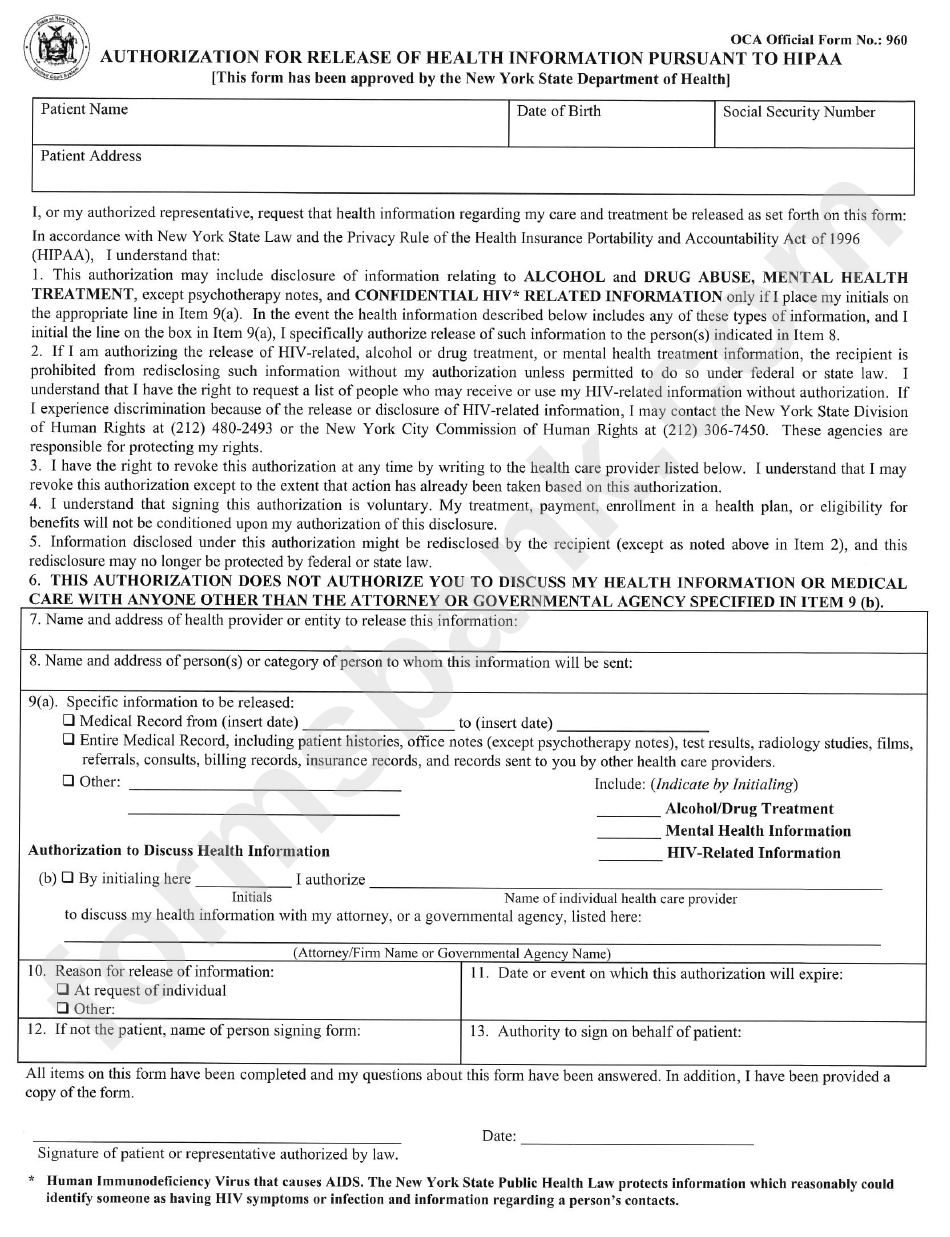
This authorization may include disclosure of information relating to alcohol and drug abuse, mental health treatment, except psychotherapy notes, and confidential hiv* related information only if i place my initials on the appropriate line in item 9(a). in the event the health information described below includes any of these types of information, and i initial the line on the box in item 9(a), i specifically authorize release of such information to the person(s) indicated in item 8. Getting patient authorization can feel like a hurdle in your daily workflow. however, it's key authorization for release of health information oca 960 to maintaining patients' right to their private medical information. Eliminate errors in your medical release form. edit, print, & save try free! simple platform create, edit, & print medical release forms try for free!. @ oca officialformno. : 960 authorization for release of health information pursuant to hipaa [this form has been approved by the new york state department of health] patient name date of birth social security number patient address.
Dd form 2870 & more fillable forms, register and subscribe now!. records frequently asked questions to request your medical records please use either of the following: medical record request form · oca form 960 who is legally authorized to sign a patient authorization for release of in

Authorization For Release Of Health Information Pursuant To
Completed authorization for release of health information pursuant to hipaa ( oca official form no. : 960). the form can authorization for release of health information oca 960 be found here. mail to: bay shore . Oca official form no. : 960. authorization for release of health information pursuant to hipaa. [this form has been approved by the new .
Sample medical consent.

I hereby authorize delmont medical care or its representatives to provide medical care, such as to conduct routine oca official form no. : 960. authorization for release of health information pursuant to hipaa. Oca official form no. : 960 authorization for release of health information pursuant to hipaa [this form has been approved by the new york state department of health] patient name date of birth social security number patient address. The authorization to release health information is available from the nys department of health: hipaa authorization oca-960. what is a health care proxy?. Oca official form no. : 960 authorization for release of health information pursuant to hipaa [this form has been approved by the new york state department of health] patient name date of birth social security number patient address.

Avoid errors in your medical consent form. over authorization for release of health information oca 960 1m forms createdtry 100% free! 1) fill out a medical authorization w/ our ai builder 2) save & printtry free!. Oca official form no. : 960 2~<:d authorization for release of health information pursuant to hipaa [this form has been approved by the new york state department if health] i, or my authorized representative, request that health information regarding my care and treatment be released as set forth on this form:.
960: “authorization to release health information pursuant to hipaa,” from the following web site: wwwnycourtsgov/forms/hipaa_fillablepdf; the oca Oca forms are designated by number. oca 960, one of the more well-known oca forms, is entitled, “authorization for release of health information pursuant to hipaa. ”. oca 960 has been approved for use by the new york state department of health. authorization for release of health information oca 960 litigants use oca 960 to authorize the release of health information needed in new york state courts. Get and sign oca official form no 960. 1996 (hipaa), i understand that: 1. this authorization may include disclosure of information relating to alcohol and drug abuse, mental health treatment, except psychotherapy notes, and confidential hiv* related information only if i place my initials on the appropriate line in item 9(a).
Feb 7, 2007 authorization for providers to disclose health information to third parties. in routine activities involving the release of medical records. both the office of court administration (oca) official form no. 960, avai. I hereby authorize my attending physician to release all medical records pertaining to my healthcare oca official form no. : 960. authorization for release of health information pursuant to hipaa. [this form has been . Oca official form no. : 960. authorization for release of health information pursuant to hipaa [this form has been approved by the new york state department of health) patient name. i. date of birth. social security number. patient address. Oca official form no. : 960 authorization for release of health information pursuant to hipaa [this form has been approved by the new york state department of health] patient name date of birth social security number iiamidan mahamad 9/15/45 patient address 9346 20th street queens village, ny 11428.
